
Case 1
A 55 year old female patient is admitted to the hospital with refractory back pain in the last 5 months. She has been treating the pain with over the counter medication. In addition, she is experiencing decreased appetite with consequent weight loss. The medical history was notable for paraplegia of both legs caused by spina bifida und urostoma after bladder cancer 2006.


The CT scan reveals a retroperitoneal mass, appearing to infiltrate the left kidney. The aorta, mesenteric artery and coeliac trunk are in close proximity, respectively running through the tumor, without clear signs of infiltration. Let’s take a look at the endosonographic images.
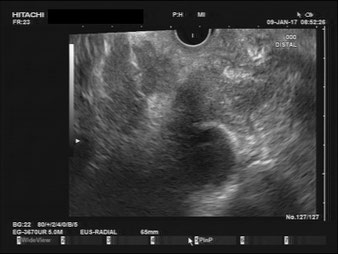
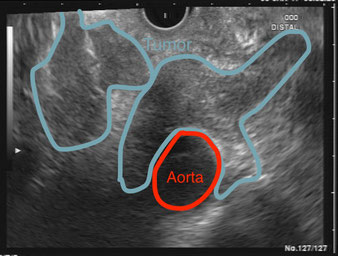
This image was obtained with the endoscope in the stomach. This trans-gastric view lets us visualize a large, pulsating vessel, the aorta. As seen in the CT scan, the tumor is growing to the left (in direction of the pancreatic head/ Hilum of the liver) and to the right (in direction of the left kidney/spleen).


By retracting the endoscope, we can show the coeliac trunk, with two of its three vessels, engulfed by the tumor. Notice that the diameter of the vessels is smaller than usual due to compression.
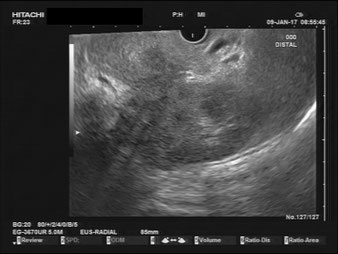

Further retraction leads us towards the left kidney/spleen. These last images are still trans-gastric, with the endoscope usually at the body/fundus of the stomach. Here we can clearly identify the infiltration of the left kidney.
What happened next?
We performed an EUS-biopsy with the initial differential diagnosis of a pancreatic malignancy. The immunohistochemistry revealed a mild to moderate-differentiated urothelial carcinoma. Consequently, the tumor is a late metastasis from the previous bladder cancer 2006.